Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 4
Open Access
Volume 4
Fanfani F1; Fagotti A1; Shah A2; Canavan K3; Veldhuis P3*; Pineda J3
*Corresponding Author: Paula Veldhuis
Ethicon, Inc, 4545 Creek Rd, Cincinnati, OH 45242, USA.
Email: PVeldhui@its.jnj.com
Article Info
Received: Oct 09, 2024
Accepted: Nov 04, 2024
Published: Nov 11, 2024
Archived: www.jclinmedsurgery.com
Copyright: © Veldhuis P (2024).
Abstract...
Background: Advanced bipolar surgical devices provide surgeons aid in achievement of hemostasis and minimize operative duration while limiting lateral thermal spread. The ENSEAL X1 Curved Jaw Tissue Sealer (X1CJ) was designed to efficiently coagulate and transect vessels, tissue and/or vascular bundles. Here we report on its use (with its accompanying Generator 11 (Gen11)) in this single-arm, prospective, observational, post-market approval study in gynecological surgery.
Methods: The primary performance endpoint was achievement of ≤ Grade 3 hemostasis intraoperatively. Secondary endpoints were surgeon’s perspectives on device usage. Subjects were followed to final visit for potential device-related Adverse Events (AEs). Collected data, including demographics, intraoperative and postoperative variables, and AEs were summarized.
Results: Thirty adult subjects (mean age of 51.6±11.8 years) completed the study. The primary procedure performed was total/subtotal hysterectomy with bilateral salpingo-oopherectomy (73.3%). Of the 109 vessels transected, the majority were 3 to 5 mm (72.5%). Hemostasis was achieved in all vessels with following scores: Grade 1 (93.6%), Grade 2 (5.5%), Grade 3 (0.9%), and no Grade 4. X1CJ was used for tasks including tissue dissection (90.0%) where surgeons reported satisfaction with its use (100%); tissue cutting (96.7%) with surgeon satisfaction of 100.0%; and tissue grasping (40.0%) with surgeon satisfaction of 91.7%. Surgeons indicated GEN11 functioned as intended and unanimously agreed that the touchscreen allowed for easy set-up and operation. One AE deemed possibly device-related was reported which resolved without surgical intervention.
Conclusion: Our study showed that in gynecological procedures, the X1CJ and accompanying GEN11 system demonstrated acceptable safety and effectiveness.
Keywords: Bipolar; ENSEAL X1; Gynecologic procedures; Hemostasis.
Citation: Fanfani F, Fagotti A, Shah A, Canavan K, Veldhuis P, et al. Usability and Performance of the Curved Jaw Tissue Sealer in Gynecological Procedures. J Clin Med Surgery. 2024; 4(2): 1172.
Introduction/Background
Advances in surgical methodologies have led to significant improvements in operational efficiency and patient outcomes. The integration of technological innovations, particularly energy-based surgical devices, has been pivotal in driving surgical advances [1,2]. In order to control intraoperative bleeding, minimize post-operative complications, and improve clinical outcomes, an ideal surgical energy device must efficiently and reliably seal and cut vessels and grasp, cut and dissect tissues. Advanced Bipolar Energy is a widely utilized form of electrosurgery in both open and Minimally Invasive Procedures (MIS). Laparoscopic surgery, in particular, has seen significant progress due to the adoption of these instruments [3]. For advanced procedures, these devices have been carefully engineered to provide surgeons with the controlled precision and the ease-of-use required to aid in the achievement of hemostasis and minimized operative duration while limiting lateral thermal spread [1,4-6].
Energy vessel-sealing systems, including ultrasonic devices, advanced bipolar technology, and combination devices have gained widespread adoption across various surgical procedures including proctectomy, colectomy, hysterectomy, splenectomy, and thyroidectomy and they have a played a crucial role in improving outcomes by reducing intraoperative blood loss and surgical times, while minimizing postoperative complications [7-9]. For example, in gynecological laparoscopic surgery, advanced bipolar devices have been widely employed and have demonstrated reduced intraoperative blood loss and decreased operative times when compared to conventional bipolar energy devices [10-12]. While advanced bipolar devices have improved clinical outcomes, achieving hemostasis remains a significant concern in laparoscopic gynecological surgical procedures being important also to preserve an unobstructed visual field and minimize the need for conversion to an open procedure.
The ENSEAL X1 Curved Jaw Tissue Sealer (X1CJ) instrument was engineered to efficiently coagulate and transect vessels (up to 7 mm in diameter), tissue and/or vascular bundles. The X1CJ has a jaw which provides uniform compression, uses electrical impedance feedback to intelligently monitor tissue conditions and modulate energy delivery, thus providing efficacious sealing while simultaneously minimizing tissue damage (Figure 1). While there is literature available to demonstrate the successful use of the X1CJ in a number of surgical arenas including breast reconstruction and thoracic procedures, there is limited available information or data regarding its use in gynecological surgery [13-15]. In the present study, we report on the performance and safety of the X1CJ when used per the Instructions For Use (IFU) in gynecological procedures.
Methods
This single-arm, prospective, observational post-market approval multi-center study was performed to establish acceptable performance and safety of the X1CJ and its accompanying generator when used in gynecological procedures per instructions for use. The study was conducted under a single protocol approved by an affiliated Institutional Review Board or Ethic Committee at each site prior to study commencement. Study sites were in Italy and the United Kingdom (ClinicalTrials.gov Identifier: NCT04763421). The study was performed in compliancewith Good Clinical Practice (GCP) and the Declaration of Helsinki (2013), as well as any other applicable local regulatory requirements.
Women were recruited for this study where the X1CJ was scheduled to be used in gynecological procedures. The primary objective of this study was to show acceptable performance and safety of the X1CJ and GEN11. Subjects were consented up to 8 weeks prior to surgery and were only considered enrolled if the device was utilized during the procedure. Enrolled subjects were followed post-operatively through discharge and again at approximately 28 days post-op.
To be considered eligible for enrollment in the study subjects had to satisfy the following inclusion criteria: >18 years of age, primary open or laparoscopic procedure in which at least one vessel was to be transected with the X1CJ, and a willingness to provide informed consent and comply with study-related evaluations and schedules. Subjects were excluded if they had any physical or psychological condition which could impair study participation, or enrollment in a concurrent trial which could impact study endpoints. Informed consent was obtained prior to enrollment. Procedures were all performed using each individual institution’s standard of care.
Device and indication
The ENSEAL X1 Curved Jaw Tissue Sealer is a sterile single-patient use advanced bipolar surgical instrument (Product Codes: NSLX125C, NSLX137C, or NSLX145C) and has previously been described [13]. It is powered by the Generator 11 (GEN11) (Ethicon, Inc., Cincinnati, OH).
Endpoints
The primary performance endpoint was the achievement of ≤ Grade 3 hemostasis intraoperatively for each vessel transected based upon the following grading scale [16]:
Grade 1: No bleeding at transection site
Grade 2: Minor bleeding at transection site, no intervention required.
Grade 3: Minor bleeding at transection site, mild intervention required (i.e., compression, monopolar device and/or touch-ups).
Grade 4: Significant bleeding (e.g., pulsatile blood flow, venous pooling) requiring intervention such as extensive coagulation or ligation with use of additional hemostatic measures.
In order to address secondary performance endpoints, surgeons were asked to complete three separate surveys (utilizing Likert-like scaled questionnaires) during the course of the study.
1. Surgeon questionnaire: Assessing surgeon’s perspectives for various device usages (adhesiolysis, lymphatics or tissue bundle division, tissue grasping, tissue cutting, or tissue dissection) were obtained. This survey was completed after the 2nd procedure completed by any given surgeon.
2. Task questionnaire: Surgeons were queried via an unvalidated tool about their perceptions of how the device performed during each procedure. The survey was completed by the Investigators after each procedure.
3. Generator questionnaire: Investigators were asked to provide insights on how the GEN11 functioned during each procedure. This survey was completed after each case.
Occurrence of Adverse Events (AEs) and Serious Adverse Events (SAEs) deemed device-related were assessed to evaluate safety. These AEs were collected over the course of the entire study period. Subjects were followed to their final visit which occurred approximately 28 (±14) days post-op to ascertain whether any further potential device-related AEs or primary procedure-related reoperations had occurred.
Data collection
Demographic data and clinical variables were obtained at baseline and included age at consent, sex, race, height, weight, Body Mass Index (BMI), ASA score, and indication for surgery. Additional compiled data included primary procedure performed and its duration, if case was converted to open, approximate vessel size transected (surgeon-approximated), any potential concomitant procedure, estimated intraoperative blood loss, other energy device utilized in the primary or concomitant procedure, need (and number) of X1CJ touchups for Grade 3, and length of stay (LOS).
Statistics
Summary statistics were performed for baseline demograp- hics and clinical data. The study summarized the number and percentage of vessels where hemostasis was achieved (≤ Grade 3). For each procedure and sub-group, an exact 95% confidence interval of hemostatic seals was estimated. The summary also included counts and percentages related to the type, size, and number of vessels transected, grading scale distribution for all vessels, the frequency of X1CJ touch-ups, and the incidence of additional measures needed for hemostasis (such as other advanced energy devices or hemostatic measures). Additionally, AEs and SAEs were reported by number and percentages.
Results
A total of thirty female subjects with a mean age of 51.6±11.8 years completed the study. Of those, the majority were pre-menopausal (63.3%) and the remainder postmenopausal (36.7%). Indications for surgery included uterine fibroids (23.3%), abnormal uterine bleeding (13.3%), endometrial cancer (13.3%), and BRCA1 mutation (13.3%) (Table 1).
The mean procedure duration was 1.5±0.45 hours with an estimated 135.3 mL blood loss. The primary procedures performed included total/subtotal hysterectomy with bilateral bilateral salpingo-oopherectomy (73.3%) and laparoscopic-assisted vaginal hysterectomy with bilateral salpingectomy (13.3%). The majority of procedures were laparoscopic (96.7%) with two conversions to open (6.9%). No calcified tissues/vessels, atherosclerotic, or vessel skeletonization was observed though some adhesions (16.7%) and fibrotic tissues (10.0%) were present. One concomitant procedure, a low pelvic/vaginal swab, was performed. No blood transfusions were given during the course of the study. All patients were discharged to home after a mean length of stay of 2.8±1.9 days (Table 2).
A total of 109 vessels were transected and the specifics are provided in (Table 3). Surgeons estimated vessel sizes with the majority being between 3 to 5 mm (72.5%), <3 mm (19.3%), and >5 to 7 mm (8.3%). 93.6% of the transections achieved a Grade 1 hemostasis, followed by Grade 2 (5.5%), Grade 3 (0.9%), and no Grade 4 (Figure 3). One vessel transected as a Grade 3 required a touch-up using the X1CJ. No clips were applied prophylactically. Of the 109 vessels transected, all of the vessel transections achieved a Grade 3 or lower hemostasis with a 95% confidence interval of 96.7%-100.0%.
The X1CJ was used for a variety of tasks including tissue dissection (90.0%) where surgeons reported satisfaction with its use (100%); tissue cutting (96.7%) with surgeon satisfaction of 100.0%; tissue grasping (40.0%) with surgeon satisfaction of 91.7%; and division of tissue bundles (40.0%; surgeon satisfaction 100%). A majority of surgeons elected to utilize an additional energy source during the primary procedure (80.0%). Surgeons indicated that the GEN11 functioned as intended and unanimously agreed that the touchscreen allowed for easy set-up and operation. A full listing of survey queries is provided in (Table 4). Results from a separate questionnaire completed by surgeons after their second case using the X1CJ found that generally there was less fatigue experienced when compared to previous devices used (75.0%) and was also easier to use (75.0%), reduced the need for instrument changes (100%), and in the most critical tasks in the case performed better (75.0%). Additionally, the separate Cut and Seal buttons (Figure 2) were easily distinguishable (100%) for all surgeons.
There was one reported possibly device-related AE during the course of the study: an intra-abdominal hemorrhage occurring one day post-operative which resolved without need for surgical intervention. Although there were four serious AEs reported during the study (abdominal pain, pelvic venous thrombosis, vaginal hemorrhage, and procedural pain), none were deemed to be device-related. No deaths occurred during the study.

Figure 1: Close-up of ENSEAL X1 curved jaw tissue sealer tip.

Figure 2: X1CJ buttons.
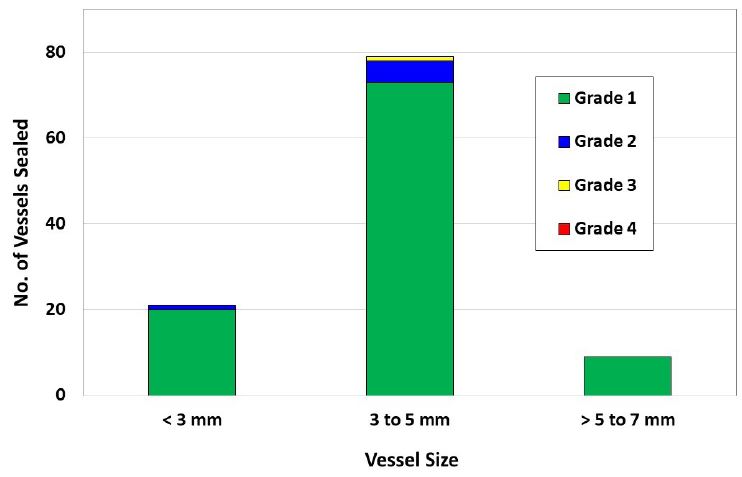
Figure 3: Hemostasis grade of vessel seals grouped by vessel size. There were no grade 4 seals.
Table 1: Baseline characteristics.
| Measure | Values |
|---|---|
| Total # of subjects | 30 |
| Age at consent (years) | |
| Mean ± SD [Median] | 51.6±11.3 [50.0] |
| Range | 33.0; 85.0 |
| Ethnicity, n(%) | |
| Hispanic or Latino | 3(10.0%) |
| Not Hispanic or Latino | 27(90.0%) |
| Race, n (%) | |
| White | 29(96.7%) |
| Asian | 1(3.3%) |
| Body Mass Index(kg/m2) | |
| Mean ± SD [Median] | 25.4 ± 4.6 [24.2] |
| Range | 19.0; 38.7 |
| ASA, n (%) | |
| I | 9(30.0%) |
| II | 19(63.3%) |
| III | 1(3.3%) |
| IV | 1(3.3%) |
| V | 0 |
| Smoking status, n (%) | |
| Current smoker | 5(16.7%) |
| Former smoker | 3(10.0%) |
| Never smoked | 22(73.3%) |
| Indication for surgery, n (%) | |
| Uterine fibroids | 7(23.3%) |
| Abnormal uterinebleeding | 4(13.3%) |
| Endometrial cancer | 4(13.3%) |
| Endometriosis | 2(6.7%) |
| BRCA 1 mutation | 4(13.3%) |
| Atypical or hyperplasic endometrium | 2(6.7%) |
| Cervical cancer | 2(6.7%) |
| Complex endometrial hyperplasia with atypia | 1(3.3%) |
| Adenocarcinoma | 1(3.3%) |
| Cervical screening abnormality | 1(3.3%) |
| Hematometra and endometriosis | 1(3.3%) |
| Cervical pre-cancer | 1(3.3%) |
Table 2: Intraoperative variables (n=30).
| Measure | Values |
|---|---|
| Primary procedure performed, n (%) | |
| Total/subtotal hysterectomy with bilateralsalpingo- oopherectomy | 22(73.3%) |
| Laparoscopic assisted vaginal hysterectomywith bilateral salpingectomy | 4(13.3%) |
| Total laparoscopic hysterectomy | 2(6.7%) |
| Laparoscopic vaginal hysterectomy | 1(3.3%) |
| Laparoscopic assisted vaginal hysterectomywith bilateral salpingo-oopherectomy | 1(3.3%) |
| Procedure duration (hours) | |
| Mean ± SD (Median) [Range] | 1.48±0.453 (1.43)[0.7; 2.5] |
| Estimated bloodloss (mL) | |
| Mean ± SD (Median) [Range] | 135.3±163.4 (50.0)[20.0; 720.0] |
| Surgical approach, n (%) | |
| Laparoscopic | 29(96.7%) |
| Open | 1(3.3%) |
| Conversion to open, n (%) | 2(6.9%) |
| Estimated uterinesize (grams) | |
| Mean ± SD (Median) [Range] | 87.0 ± 39.8 (90.0) [45.0; 123.0] |
| Vessel skeletonization? | 3(10.0%) |
| Prophylacticuse of clipsas standard of careprior to vessel transection? | 0(0%) |
| Presence of Inflamed tissue/Vessels? | 1(3.3%) |
| Presence of atherosclerotic tissue? | 0(0%) |
| Presence of fibrotic tissues? | 3(10%) |
| Presence of adhesions? | 5(16.7%) |
Table 3: Skeletonization and transection summary.
| Name of vesseltransected | n (%) |
|---|---|
| Left uterine artery | 25(22.9%) |
| Right uterineartery | 22(20.2%) |
| Left uterine vein | 13(11.9%) |
| Right uterinevein | 13(11.9%) |
| Right ovarian vein | 5(4.6%) |
| Left ovarianartery | 4(3.7%) |
| Left ovarianvein | 4(3.7%) |
| Right ovarian artery | 4(3.7%) |
| Other | 19(17.4%) |
Table 4: X1CJ and GEN11 usage survey results.
| Measure | Value |
|---|---|
| X1CJ usability survey | |
| Number adhesions removed or divided withX1CJ | 8/30(26.7%) |
| Percent satisfied with adhesion removalor division | 8/8(100%) |
| Number lymphatic bundles divided by X1CJ | 2/30(6.7%) |
| Percent satisfied withlymphatic bundle division | 2/2(100%) |
| Number tissue bundles divided by X1CJ | 12/30(40.0%) |
| Percent satisfied withtissue bundles division | 12/12(100%) |
| Number times X1CJ used for tissue grasping | 12/30(40.0%) |
| Percent satisfied withtissue grasping | 11/12(91.7%) |
| Number times X1CJ used for tissue cutting | 29/30(91.7%) |
| Percent satisfied withtissue cutting | 29/29(100%) |
| Number times X1CJ used for tissue dissection | 27/30(90.0%) |
| Percent satisfied withtissue dissection | 30/30(100%) |
| Number times any other energydevice was usedduringprocedure | 24/30(80.0%) |
| Type of otherenergy device used: | |
| Monopolar | 4/24(16.7%) |
| Traditional Bipolar | 20/24(83.3%) |
| GEN11survey | |
| Software version used | |
| 2016-1 | 5/30(16.7%) |
| 2016-1.1 | 24/30(80.0%) |
| Other | 1/30(3.3%) |
| Number timessurgeons reported touchscreen allowed for easy set-up and operation | 30/30(100%) |
| Number of generator-related alarms | 0/30(0.0%) |
| Number of timesgenerator performed as intended | 30/30(100%) |
Discussion
Hemostasis has been a recurrent primary endpoint in several studies evaluating advanced bipolar devices [11,13,17]. This may be in part due to the severity of complications which can arise if bleeding is not promptly and thoroughly addressed, such as arrythmias, myocardial infarctions, and overall increased mortality [18]. Our study employed a validated hemostasis grading scale that has been used in several device evaluations [16].
In a prior similar post-market analysis of the ENSEAL X1 Large Jaw device, on open gynecological procedures, even though hemostasis was overall satisfactory, between gynecological, thoracic, and colorectal procedures, the gynecological procedures had the lowest percentage score of hemostasis grade 3 and below (94%, 96%, 100%) [17]. However, even though there was a lower hemostasis score, total blood loss was commensurate with already published literature on typically reported blood loss. This finding was assumed to be due to the technical difficulty of accessing the deep pelvic space and nature of disease and not necessarily device related [17-20].
Several differences in the current X1CJ device being evaluated compared to the previous study of Enseal X1 Large jaw include jaw size, distal tip compression and electrode configuration. Ideally, advancements in device engineering should include refinement in instrument control in order to achieve more precise tissue manipulation, dissection, and hemostasis. In our study less than 1% of patients were identified having a Grade 3 bleed and there were no Grade 4 bleeds.
Advanced bipolar devices are utilized across the spectrum of surgical fields including those that implement minimally invasive techniques. In the study presented here, the majority of cases were MIS though one case was open and there were 2 conversions to open. The gynecologic field has been progressively adopting more minimally invasive surgical technologies. When evaluating surgical tasks when using the X1CJ surgeons reported 100% satisfaction with tissue dissection, cutting, and division of tissue bundles and 91% of surgeons were satisfied with tissue grasping. Most surgeons (80%) used an additional energy source (traditional bipolar 83.3%; monopolar 16.7%). Despite no additional information was collected, it is the author’s assumption that the additional source of energy was a monopolar device used to create the access to the abdominal cavity. Additionally, most surgeons (80%) reported that the Gen 11 generator functioned as intended.
In this study, 75% of surgeons reported that the X1CJ was easier to use and that they experienced less fatigue than with their previous devices used for similar tasks. Of note, all surgeons (100%) agreed that there was less need for instrument exchange needed during procedures. Performing surgery can be physically taxing [21]. Thus, easy-to-use, well-designed instruments result in overall less fatigue during surgery and are vital considerations for device selection by surgeons.
One limitation of this study is the small sample size but is appropriate given this is a small observational study. Further studies are important to confirm what we report here.
Conclusion
Our study provides evidence that in gynecological procedures, the X1CJ and accompanying GEN11 system demonstrate acceptable safety and effectiveness. Of note, hemostasis was achieved in all vessels sealed. Additionally, the majority of surgeons reported reduced fatigue, ease of use, and decreased need for instrument changes when utilizing the device.
Declarations
Financial support and competing interests: Study sites (FF, AF, AS) were funded by Ethicon, Inc. (Cincinnati, OH) for study conduct. KC, PV, and JP are employees of Ethicon, Inc., Cincinnati, OH. No other conflicts of interest were reported by authors.
Ethical approval: Institutional Review Board or Ethics Committee approval was received by each participating site prior to study onset. FF and FA approvals were received by Comitato Etico Dell Universita Cattolica Del s Cuore, Policlinico Gemelli, Roma, ITALY, Approval # 3608. The site associated with AS received approval from London Dulwich Research Ethics Committee, London, UK, IRAS Approval # 286688.
Author contribution: Conception and design of work was performed by FF, AF, AS. The following were instrumental in data collection, ensuring its integrity and accuracy: FF, AF, AS, KC. All authors were involved in data analysis and interpretation: FF, AF, AS, KC, PV, JP. The manuscript was drafted by PV and all authors provided critical review and possible revision of manuscript. All authors approved the final version: FF, AF, AS, KC, PV, JP.
References
- Olasehinde O, Owojuyigbe A, Adeyemo A, et al. Use of energy device in general surgical operations: Impact on peri-operative outcomes. BMC Surg. 2022; 22(1): 90.
- Vettoretto N, Foglia E, Gerardi C, et al. High-energy devices in different surgical settings: Lessons learnt from a full health technology assessment report developed by SICE (Società Italiana di Chirurgia Endoscopica). Surgical endoscopy. 2023; 37(4): 2548-2565.
- El-Sayed MM, Saridogan E. Principles and safe use of electrosurgery in minimally invasive surgery. Gynecology and Pelvic Medicine. 2020; 4.
- Patrone R, Gambardella C, Romano RM, et al. The impact of the ultrasonic, bipolar and integrated energy devices in the adrenal gland surgery: Literature review and our experience. BMC Surgery. 2019; 18(1): 123.
- Grochola LF, Vonlanthen R. Surgical Energy Devices or Devices for Hemostasis. In: Clavien P-A, Sarr MG, Fong Y, Miyazaki M, eds. Atlas of Upper Gastrointestinal and Hepato-Pancreato-Biliary Surgery. Berlin, Heidelberg: Springer Berlin Heidelberg. 2016: 37-44.
- Shibao K, Honda S, Adachi Y, et al. An advanced bipolar device helps reduce the rate of postoperative pancreatic fistula in laparoscopic gastrectomy for gastric cancer patients: A propensity score-matched analysis. Langenbeck’s archives of surgery. 2022; 407(8): 3479-3486.
- Wael A, Mohamed Rifaat A, Aly S. Use of Ligasure Sealing Versus Conventional Suture - Ligation in Total Thyroidectomy. Journal of Surgery. 2016; 4(3-1): 34-38.
- Charalambides M, Afxentiou T, Pellino G, et al. A systematic review and network meta-analysis comparing energy devices used in colorectal surgery. Tech Coloproctol. 2022; 26(6): 413-423.
- Madani A, Mueller CL. Fundamentals of Energy Utilization in the Operating Room. In: Palazzo F, ed. Fundamentals of General Surgery. Cham: Springer International Publishing. 2018: 129-136.
- El-Sayed M, Mohamed S, Saridogan E. Safe use of electrosurgery in gynaecological laparoscopic surgery. The Obstetrician & Gynaecologist. 2020; 22(1): 9-20.
- Abi Antoun M, Etrusco A, Chiantera V, et al. Outcomes of conventional and advanced energy devices in laparoscopic surgery: a systematic review. Minimally invasive therapy & allied technologies: MITAT: Official journal of the Society for Minimally Invasive Therapy. 2024; 33(1): 1-12.
- Zorzato PC, Ferrari FA, Garzon S, et al. Advanced bipolar vessel sealing devices vs conventional bipolar energy in minimally invasive hysterectomy: A systematic review and meta-analysis. Archives of gynecology and obstetrics. 2024; 309(4): 1165-1174.
- Singleton D, Ricketts C, Boguszewski D, Cummings J, Lewis K, et al. Effectiveness and Useability of a Newly Designed Advanced Bipolar Tissue Sealer, ENSEAL X1 Curved Jaw Tissue Sealer. World J Surg Surgical Res. 2021; 4: 1304.
- Takimoto A, Fumino S, Takayama S, et al. Laparoscopic resection of pediatric interaortocaval large paraganglioma. Journal of Pediatric Surgery Case Reports. 2022; 78: 102195.
- Tomita K, Taminato M, Kubo T. Total breast reconstruction with a fat-augmented latissimus dorsi flap: A comparative study between muscle and myocutaneous flaps. Journal of Plastic, Reconstructive & Aesthetic Surgery. 2023; 83: 250-257.
- Siegel JM, Cummings JF, Clymer JW. Reproducible, repeatable and clinically-relevant hemostasis scoring. Journal of Advances in Medical and Pharmaceutical Sciences. 2014; 1(1): 30-39.
- Schilder J, Anderson D, Shah F, et al. Hemostatic efficacy of an advanced bipolar sealer in open gynecologic, thoracic, and colectomy procedures: A prospective cohort study. International Journal of Surgery Open. 2020; 24: 57-63.
- Carson JL, Noveck H, Berlin JA, Gould SA. Mortality and morbidity in patients with very low postoperative Hb levels who decline blood transfusion. Transfusion. 2002; 42(7): 812-818.
- Sallam HF, Shady NW. Reducing Blood Loss During Abdominal Hysterectomy with Intravenous Versus Topical Tranexamic Acid: A Double-Blind Randomized Controlled Trial. Journal of obstetrics and gynaecology of India. 2019; 69(2): 173-179.
- Uccella S, Morosi C, Marconi N, et al. Laparoscopic Versus Open Hysterectomy for Benign Disease in Uteri Weighing >1 kg: A Retrospective Analysis on 258 Patients. J Minim Invasive Gynecol. 2018; 25(1): 62-69.
- Wells AC, Kjellman M, Harper SJF, Forsman M, Hallbeck MS. Operating hurts: A study of EAES surgeons. Surgical endoscopy. 2019; 33(3): 933-940.